Choosing MedCon Benefit Systems Group, Inc. as your benefits broker – we aim to improve your bottom line and save you money – all at the same time.
We understand you need to save money on employee benefits.
With the rising cost of employee benefits, balancing employee needs with your capabilities and bottom line has never been more difficult. Let us help you meet your benefits goals, your employees’ expectations and your bottom line.
MedCon provides not only insurance, but also employee benefits consulting services. We save you money by delivering benefits solutions that meet your needs through strategic planning, professional services and technology-based solutions.
What You Should Expect from Your Insurance Broker
Your broker shouldn’t stop at obtaining competitive quotes for coverage and handling claims issues—you should expect more from your insurance broker.
MedCon goes above and beyond, providing quality service throughout the year. From custom employee communication materials to human resources tools and claims data analysis, we have the tools to make your benefits goals a reality.
The bare minimum doesn’t cut it anymore—get what you really need from your insurance broker.
Officially Obtaining Our Firm’s Services
There is no standard contract to sign to obtain services from an insurance broker. MedCon is an independent agency that works with a wide variety of carriers in order to provide you with the best possible benefits options.
Once you have chosen us as your insurance broker, you need only provide your current carriers with a letter establishing us as your broker of record. We even provide this letter for you—if you would like to see a sample, please let us know.
When we are established as your broker of record, we are able to do a detailed market analysis, getting quotes from more markets, better leveraging our relationships with carriers and taking advantage of a better negotiating position with carriers.
Increase Value, Not Cost
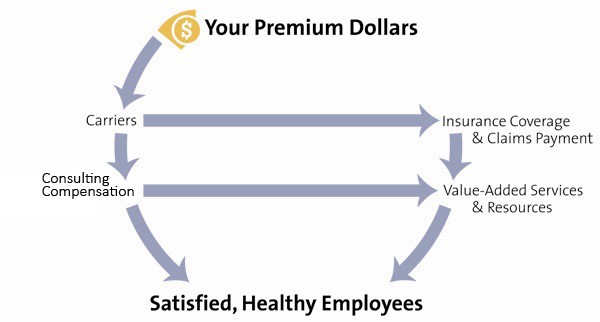
Providing the best possible value and service to your employees is important—especially because they are paying a portion of the benefits costs and our commission.
While some brokers only provide quotes, we also provide clear and professional enrollment materials, wellness communication materials and other resources to help keep employees healthy and safe.
Saving You Money
The value-added services we offer can save your employees money and protect your bottom line. The educational materials we provide can do everything, from helping employees understand their health care needs to enabling them to make healthy lifestyle changes. Helping employees understand the benefits that are available and make educated decisions about which benefits are right for them allows them more say in their health care, and also saves you money.
Employees educated on the importance of preventive care may be less likely to rack up hospital bills resulting from leaving conditions untreated. Employees with large families and frequent doctor visits may choose a health plan with broader coverage than employees who live alone and visit the doctor infrequently.
Allowing employees to choose the level of coverage that is right for them saves you money in the short and long term.
Contact MedCon Benefit Systems Group, Inc. today to learn more about the value we can bring to your organization – we look forward to partnering with you!
